Ulnar Collateral Ligament (UCL) Reconstruction (Tommy John surgery)
Anatomy
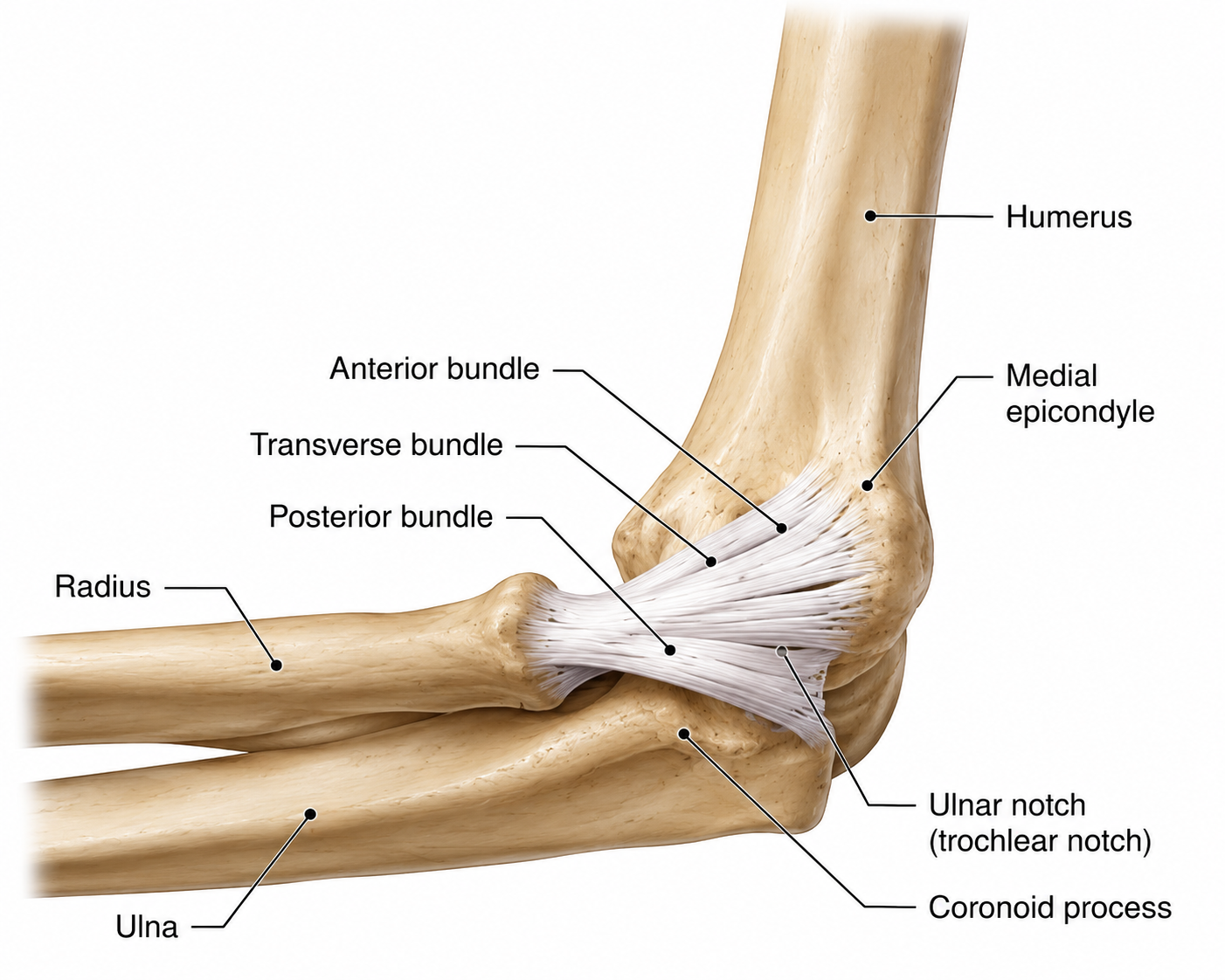
The elbow is a joint formed by three bones: the humerus in the upper arm, and the radius and ulna in the forearm. It allows two types of movement: bending and straightening the arm, and rotating the forearm to turn the palm up or down. The joint is stabilized by ligaments on both sides. On the inner side is the ulnar collateral ligament (UCL). On the outer side is the lateral collateral ligament (LCL).
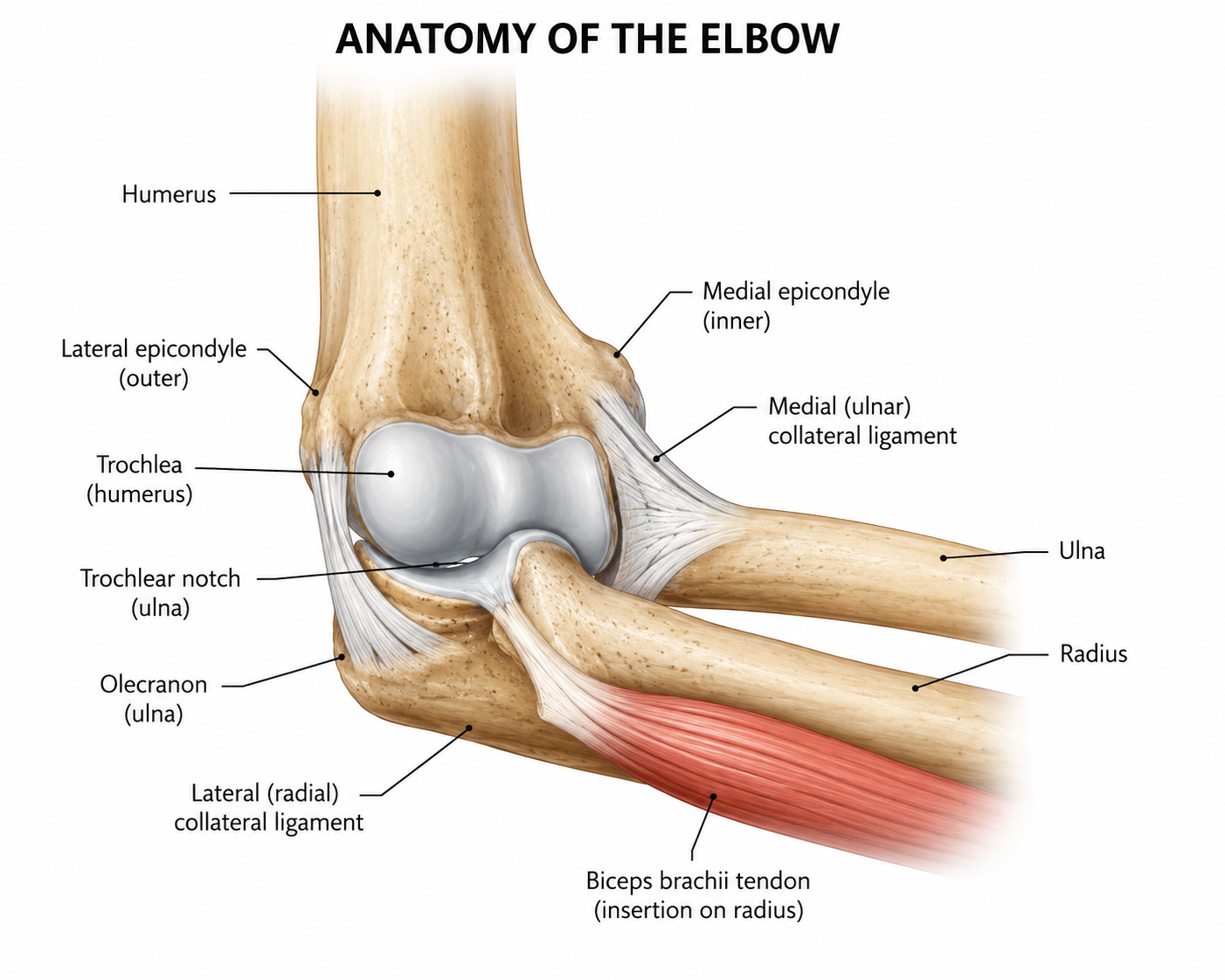
Several muscle groups cross the elbow. The biceps and brachialis bend the elbow, and the triceps straighten it. The forearm muscles that move the wrist and fingers also attach at the elbow, at bony points called the medial and lateral epicondyles. The medial epicondyle is on the inner side, where the ulnar nerve passes close to the surface. The lateral epicondyle is on the outer side, where the wrist extensor muscles attach.
UCL Tears
The ulnar collateral ligament, or UCL, runs along the inner side of the elbow and connects the humerus to the ulna. Its main job is to resist valgus stress: the outward force placed on the elbow when the arm is used overhead or in throwing motions. UCL tears are most common in overhead athletes, particularly baseball pitchers, because of the repetitive stress placed on the ligament with every throw. The tear can happen suddenly from a single forceful movement or gradually over time as the ligament breaks down from accumulated stress.
The most common symptom is pain on the inner side of the elbow, often felt during or after throwing. Some people notice a “pop” at the moment of injury. Instability is another common complaint. In some cases, the ulnar nerve is affected, causing tingling or numbness in the ring and pinky fingers.
Treatment Options
Non-Operative Treatments
Rest and Activity Modification: Initial treatment for a torn UCL often begins with a period of rest from throwing or overhead activities that place stress on the elbow. Activity modification helps reduce inflammation, minimize further injury, and allows the ligament an opportunity to heal naturally.
Physical Therapy and Rehabilitation: A structured rehabilitation program focuses on restoring elbow range of motion, improving flexibility, and strengthening the muscles surrounding the shoulder, forearm, and core. Improving overall arm mechanics can reduce stress placed on the UCL during athletic activity.
Anti-Inflammatory Medications: Nonsteroidal anti-inflammatory medications (NSAIDs) may be used to help decrease pain and inflammation associated with a UCL injury. These medications are often combined with rest and therapy during the early stages of recovery.
Bracing or Elbow Support: In some cases, an elbow brace may be recommended to limit excessive stress across the joint during healing. Functional bracing can also provide additional stability during gradual return-to-play progression.
Platelet-Rich Plasma (PRP) Injections: PRP therapy involves injecting concentrated platelets derived from the patient’s own blood into the injured ligament. The goal is to stimulate healing and improve tissue recovery, particularly in partial UCL tears.
Surgical Options
Tommy John Surgery (UCL Reconstruction): The most well-known surgical intervention for ulnar collateral ligament tears is UCL reconstruction, commonly referred to as Tommy John surgery. In this procedure, the damaged ligament is replaced with a tendon graft harvested from another part of the patient's body.
Recovery is extensive, typically requiring 12 to 18 months before an overhead-throwing athlete can return to full competitive activity.
Dr. Tingstad specializes in UCL injuries and will help you select the best treatment based on your injury.