Shoulder Tendonitis
Anatomy
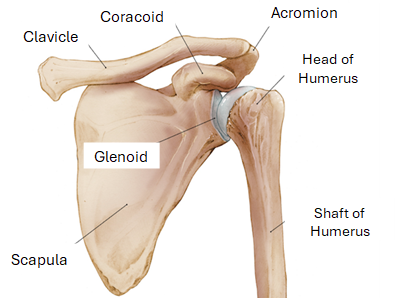
The shoulder is a ball-and-socket joint, meaning a rounded head fits into a cupped depression, allowing for a wide range of motion.
The shoulder is primarily made up of three main bones:
The Humerus: is the upper portion of the arm and is rounded at the top. The top end is rounded and forms the ball of the ball-and-socket joint.
The Scapula: or the shoulder blade, is the large, flat, triangular bone on the back of the shoulder/chest. The part of the scapula that forms the socket is called the glenoid.
The Glenoid: This is the “socket” part. It is relatively shallow, which allows for a lot of movement but also makes the joint less stable compared to the hip.
The Clavicle: also known as the collarbone, is the bone that connects the sternum (breastbone) to the shoulder blade, providing structural support.
Supporting Structures
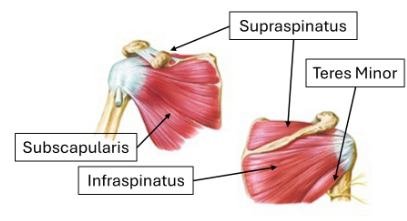
The Rotator Cuff: is a group of four muscles and their tendons that surround the joint. They act like a dynamic sling, holding the ball of the humerus centered in the shallow glenoid socket. This allows you to rotate and lift your arm.
Cartilage: a smooth, gliding tissue that covers the ends of the bones (the head of the humerus and the glenoid). This allows the bones to glide against each other easily and without pain. When this cartilage wears out, you get arthritis, which is often what leads to a total shoulder replacement.
What is Shoulder Tendonitis?
Shoulder tendonitis is inflammation of one or more tendons in the shoulder, most commonly affecting the rotator cuff or the biceps tendon. It typically develops from repetitive overhead motions, such as those involved in swimming, painting, throwing sports, or certain manual labor jobs, which cause the tendon to become irritated and swollen over time.
Age-related wear and tear can also play a role, as tendons naturally lose elasticity and become more prone to injury as people get older. Common symptoms include a dull ache deep in the shoulder, pain that worsens with movement or at night, and stiffness or weakness when lifting the arm.
Treatment Options
Non-Operative Treatments
Rest and activity modification: avoiding the repetitive or overhead movements that aggravate the tendon
Ice therapy: applying ice for 15-20 minutes several times a day to reduce inflammation and pain
NSAIDs: over-the-counter or prescription anti-inflammatory medications like ibuprofen or naproxen
Physical therapy: targeted exercises to strengthen the rotator cuff and surrounding muscles, improve flexibility, and correct posture or movement patterns
Corticosteroid injections: used for more persistent pain when other measures haven't provided enough relief
Surgical Options
Arthroscopic debridement: A minimally invasive procedure that removes damaged or inflamed tendon tissue using small instruments and a camera (arthroscope) inserted through tiny incisions.
Subacromial decompression: The surgeon removes a small portion of bone or tissue under the acromion to create more space and relieve pressure on the rotator cuff tendons.
Rotator cuff repair: The surgeon reattaches the torn tendon to the bone, often done arthroscopically.
Biceps tenodesis or tenotomy: For biceps tendon involvement, the surgeon either reattaches the tendon to a new location (tenodesis) or releases it entirely (tenotomy) to relieve pain.
Open surgery: This is a more invasive approach with a larger incision, typically reserved for cases where arthroscopic techniques aren't suitable.
Distal clavicle excision: The surgeon removes the small portion of the collarbone contributing to impingement and tendon irritation.
Dr. Tingstad specializes in shoulder tendonitis and will work with you to find the best treatment option for your shoulder.