Rotator Cuff Repair
Anatomy
The shoulder is made up of three bones: the humerus, scapula (shoulder blade), and clavicle (collar bone).
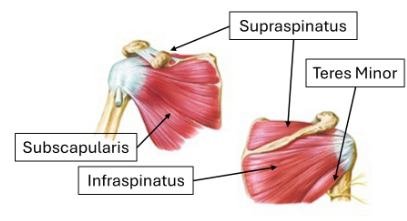
The rotator cuff is a group of four muscles (supraspinatus, infraspinatus, subscapularis, and teres minors) that attach to the humeral head. The supraspinatus comes over the top of the humerus and attaches via a tendon into the humerus. It is typically the tendon portion that tears or wears away.
The acromion and distal clavicle are bony structures that overlie the rotator cuff and serve as attachments for muscles, forming the acromioclavicular joint.
Rotator Cuff Tears
Most rotator cuff tears do not cause pain, and many patients are unaware of them. Rotator cuff tears are divided into partial- and full-thickness tears.
Partial tears are more common in younger patients and have variable rates of progression. However, once torn, the rotator cuff has little capacity to heal (90% will not) because many parts of the cuff have marginal blood supply.
Full-thickness tears progress faster in younger patients.
Common symptoms of a rotator cuff tear include: pain, weakness, limited mobility, and difficulty with overhead activities.
Treatment Options
Pain relief with acetaminophen, anti-inflammatories, heat and/or ice
Infrequent injections under ultrasound or x-ray guided
Restoring range of motion and surrounding strength with the use of physical therapy
Stretching
Non-Operative Options
Surgical Treatment
The natural history of rotator cuff tears is that they progressively enlarge over time. The tendon pulls further away from its bony attachment, and the muscle is replaced with fat. The rate of progression is variable, but surgical treatment of small tears consistently shows better results than treatment for large tears. Over time, some tears become irreparable and can lead some patients to develop significant degenerative osteoarthritis.
Surgery repairs the torn rotator cuff tendon(s) back to the bony attachment on the humerus.
The entire shoulder is evaluated at the time of surgery, and this is typically done arthroscopically through “poke hole” incisions.
Often a smoothing of the bony and cartilage structures is carried out at the time of surgery.
The success of surgery is dependent on many factors such as tear size, age of tear, and medical comorbidities (i.e., smoking, diabetes, etc.).
Most studies suggest that satisfactory outcomes are seen in 70-95% of cases, with an average of 85%.
Dr. Tingstad specializes in rotator cuff repairs and will help you select the best treatment based on your injury.