Reverse Total Shoulder Arthroplasty (Replacement)
Anatomy
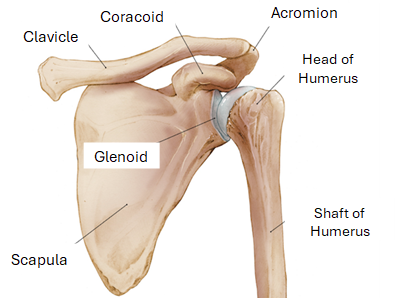
The shoulder is a ball-and-socket joint, meaning a rounded head fits into a cupped depression, allowing for a wide range of motion.
The shoulder is primarily made up of three main bones:
The Humerus: is the upper portion of the arm and is rounded at the top. The top end is rounded and forms the ball of the ball-and-socket joint.
The Scapula: or the shoulder blade, is the large, flat, triangular bone on the back of the shoulder/chest. The part of the scapula that forms the socket is called the glenoid.
The Glenoid: This is the “socket” part. It is relatively shallow, which allows for a lot of movement but also makes the joint less stable compared to the hip.
The Clavicle: also known as the collarbone, is the bone that connects the sternum (breastbone) to the shoulder blade, providing structural support.
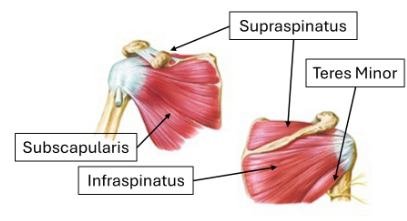
Supporting Structures
The Rotator Cuff: is a group of four muscles and their tendons that surround the joint. They act like a dynamic sling, holding the ball of the humerus centered in the shallow glenoid socket. This allows you to rotate and lift your arm.
Cartilage: a smooth, gliding tissue that covers the ends of the bones (the head of the humerus and the glenoid). This allows the bones to glide against each other easily and without pain. When this cartilage wears out, you get arthritis, which is often what leads to a total shoulder replacement.
Treatment Options
Currently, no cure for osteoarthritis exists. Surgical procedures such as a total shoulder arthroplasty resurface degenerative joint surfaces and cartilage within the joint. Non-operative treatment options can be used in some cases to manage the symptoms of osteoarthritis.
Corticosteroid or biologic injections provide temporary pain relief by reducing inflammation and improving the body’s ability to manage the inflammation in the joint.
A corticosteroid injection can be trialed prior to discussing shoulder replacement surgery. Effects can last for extended periods of time, although the injections have diminishing returns over time.
For accuracy, injections are guided by fluoroscopy (similar to x-ray) or ultrasound to ensure the corticosteroid is injected into the joint space.
Physical therapy is recommended to increase your range of motion and coordination of muscles to better support the shoulder. Priming these areas prior to surgery has been shown to improve outcomes after surgery, and some insurances require it before authorizing a total shoulder arthroplasty.
NSAID/anti-inflammatory medications such as Meloxicam or Relafen can provide pain relief and decrease inflammation in the shoulder.
Non-Operative Options
A total shoulder arthroplasty or shoulder replacement is the relining or resurfacing of the joint with artificial components called prostheses:
Shoulder replacements began in the 1950s to treat severe fractures, and by the late 1970s to early 1980s, shoulder replacements were being performed regularly to treat conditions such as osteoarthritis and later for rotator cuff insufficiency.
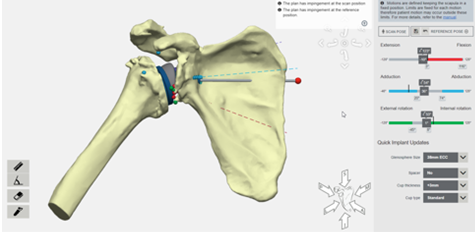
Modern shoulder replacements utilize software assistance to devise precise individualized treatments. The software overlays your anatomy for specific recommendations in placement and sizing.
Recent data from the Journal of Shoulder and Elbow Surgery in 2023 suggests that 80-90% of patients who underwent TSA were pleased with their outcome at 10+ years post-surgery.
What is a Total Shoulder Arthroplasty (TSA)?
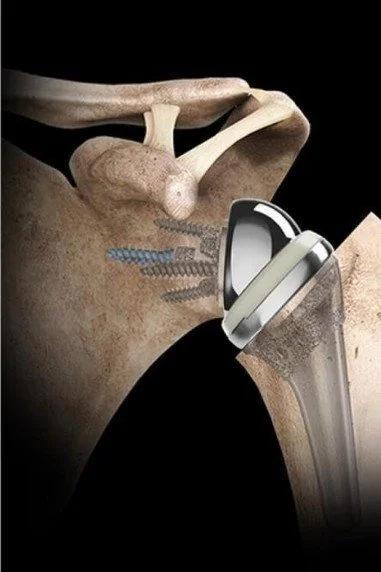
Reverse Total Shoulder Arthroplasty(rTSA)
Reverse total shoulder arthroplasty (rTSA) is a replacement similar to an anatomic TSA. However, the anatomy of the shoulder is reversed. This means the ball is placed where the socket is normally, and the socket replaces the ball.
Patients who have osteoarthritis in addition to advanced wear-and-tear in the ligaments surrounding the joint and rotator cuff are good candidates for an rTSA.
This is because in a normal shoulder, the tendons and muscles that comprise the rotator cuff are responsible for holding and moving the ball and socket. When the anatomy is reversed, the balance of tendons and muscles is no longer required to hold the joint in place.
This allows for movement of the shoulder to be controlled by the deltoid muscle.
This type of replacement does have more restrictions after surgery, but it is the most effective way to improve pain and stiffness in shoulders that have additional wear in the rotator cuff.